


If you’ve been coding for a while, you know pancreatitis is one of those conditions that looks simple on the surface — inflammation of the pancreas, right? — but turns into a rabbit hole the moment you open the codebook.
Is it acute or chronic? What caused it? Is there necrosis? Is that necrosis infected? Did the physician actually say any of this in the note, or are you left guessing? And if you get it wrong, you’re either leaving DRG reimbursement on the table or setting your organization up for an audit.
This guide cuts through all of that. We’re going code by code, scenario by scenario — with the kind of practical insight you’d get from a senior CPC sitting next to you, not a textbook definition.
| Quick Summary: The short version: Pancreatitis lives under K85 (acute) and K86 (chronic/other) in Chapter 11 of ICD-10-CM. Every billable code needs five characters. K85.9 is a dead end — never submit it on a claim. The fifth digit tells the payer how serious things got. That’s the whole game. |
A quick clinical picture — because context makes coding easier
You don’t need to be a gastroenterologist to code pancreatitis well. But understanding the basics keeps you from making assumptions that lead to wrong codes.
The pancreas is a gland sitting just behind the stomach. It does two big things: it makes digestive enzymes (exocrine function) and it regulates blood sugar through insulin and glucagon (endocrine function). When something goes wrong — a gallstone blocking the bile duct, too much alcohol, a medication reaction, trauma — those digestive enzymes start attacking the pancreas itself. That’s pancreatitis.
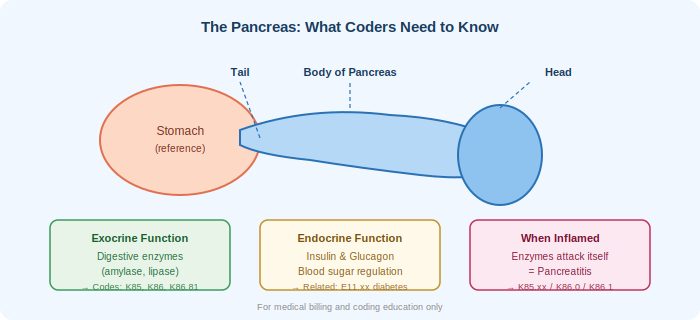
Acute pancreatitis comes on suddenly. Most of the time it resolves within a week with supportive care. But when it turns severe — when parts of the pancreas start dying (necrosis), especially if bacteria get in there (infected necrosis) — you’re looking at multi-organ failure, ICU admissions, and significantly higher reimbursement complexity.
Chronic pancreatitis is a different beast entirely. It’s not just ‘repeated episodes of acute.’ It’s progressive, irreversible damage — scarring, calcification, loss of function — that builds up over years, usually from long-term alcohol use or other persistent triggers.
Where pancreatitis sits in ICD-10-CM
Before we go code by code, here’s the filing address:
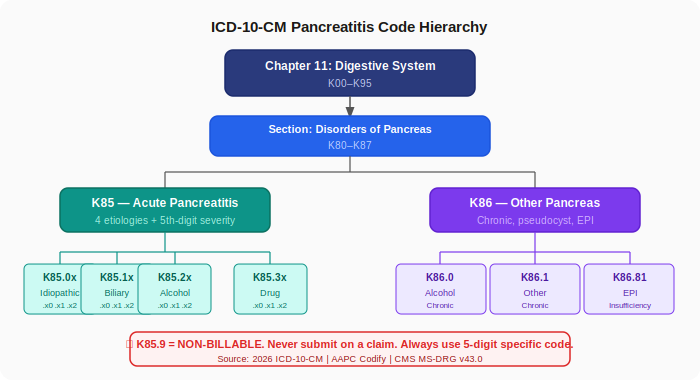
- Chapter 11 — Diseases of the Digestive System (K00–K95)
- Section K80–K87 — Disorders of Gallbladder, Biliary Tract, and Pancreas
- K85 — Acute Pancreatitis (and its subtypes)
- K86 — Other Diseases of Pancreas (chronic pancreatitis, pseudocysts, insufficiency)
The fifth digit — the most important character you’re probably missing
Before we dive into individual codes, you need to understand the fifth-digit extension that appears on every K85 code. This is where a lot of billers stumble, and it’s also where a lot of DRG value gets left on the table.
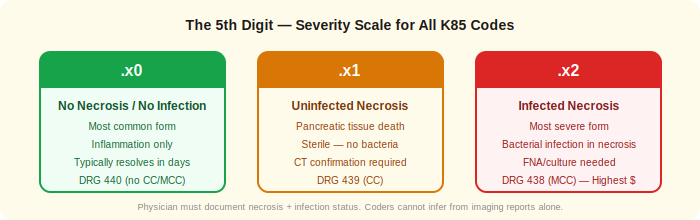
| .x0 | Without necrosis or infection — Most common form. Inflammation only. Typically resolves in days. Maps to DRG 440. |
| .x1 | With uninfected (sterile) necrosis — Pancreatic tissue has died but no bacterial infection. Confirmed by contrast-enhanced CT. Maps to DRG 439. |
| .x2 | With infected necrosis — Most severe. Bacteria in necrotic tissue. Confirmed by FNA culture or clinical picture. Maps to DRG 438 — highest reimbursement. |
| Important: Coder’s rule: You cannot assign .x1 or .x2 on your own. The attending physician must document necrosis in the record. If the CT report shows necrosis but the physician note doesn’t address it, send a query — don’t code from the radiology report alone. |
K85 — Acute Pancreatitis: Code by Code
K85.0x — Idiopathic Acute Pancreatitis
“We looked everywhere. We couldn’t find the cause.”
This is the code for when the clinical team ran a full workup — ultrasound, labs, medication review, detailed history — and still couldn’t pin down why the pancreas inflamed. ‘Idiopathic’ means unknown cause, and it has to be earned through investigation, not assigned by default because no one documented the cause yet.
| Code | Description | Billable |
| K85.00 | Idiopathic acute pancreatitis without necrosis or infection | ✓ Yes |
| K85.01 | Idiopathic acute pancreatitis with uninfected necrosis | ✓ Yes |
| K85.02 | Idiopathic acute pancreatitis with infected necrosis | ✓ Yes |
| Coder Note: Don’t default here too quickly. Idiopathic pancreatitis is a legitimate diagnosis — but it should reflect a genuine diagnostic conclusion, not a documentation gap. If the workup wasn’t completed or documented, query the physician before assigning K85.00. |
K85.1x — Biliary Acute Pancreatitis
A gallstone escapes the gallbladder and lodges at the ampulla of Vater, blocking the common bile duct and the pancreatic duct simultaneously. The backed-up pressure triggers the enzyme cascade. This is one of the most common reasons people end up hospitalized with pancreatitis, and it almost always requires a follow-up procedure — ERCP or cholecystectomy — which opens up additional CPT coding opportunities.
| Code | Description | Billable |
| K85.10 | Biliary acute pancreatitis without necrosis or infection | ✓ Yes |
| K85.11 | Biliary acute pancreatitis with uninfected necrosis | ✓ Yes |
| K85.12 | Biliary acute pancreatitis with infected necrosis | ✓ Yes |
| Billing Tip: Sequencing note: When both cholelithiasis and acute pancreatitis are present, you can code both conditions. Check NCCI edits when an ERCP or cholecystectomy is performed in the same encounter — correct sequencing of the principal diagnosis affects DRG assignment and reimbursement. |
K85.2x — Alcohol-Induced Acute Pancreatitis
Here’s where a lot of coders get caught. A patient has a history of heavy alcohol use and presents with pancreatitis. It feels obvious to reach for K85.2x — but ‘history of alcohol use’ and ‘alcohol caused this episode of pancreatitis’ are two different clinical statements, and ICD-10-CM requires the second one.
The attending physician must explicitly link the alcohol to the current episode. If the note says ‘pancreatitis, known alcohol use’ without a causative statement, you do not have sufficient documentation for K85.2x. Query the physician.
| Code | Description | Billable |
| K85.20 | Alcohol-induced acute pancreatitis without necrosis or infection | ✓ Yes |
| K85.21 | Alcohol-induced acute pancreatitis with uninfected necrosis | ✓ Yes |
| K85.22 | Alcohol-induced acute pancreatitis with infected necrosis | ✓ Yes |
| Add-on Code: When alcohol use disorder is documented, add the appropriate F10.xx code. This accurately represents the clinical picture and can contribute to comorbidity capture that affects DRG weight. |
K85.3x — Drug-Induced Acute Pancreatitis
Medications are an underappreciated cause of pancreatitis. Common culprits include thiazide diuretics, azathioprine, valproic acid, 6-mercaptopurine, and statins. When the physician documents a specific drug as the cause, you have two coding obligations — the pancreatitis code and the adverse effect code from the T36–T50 range.
| Code | Description | Billable |
| K85.30 | Drug-induced acute pancreatitis without necrosis or infection | ✓ Yes |
| K85.31 | Drug-induced acute pancreatitis with uninfected necrosis | ✓ Yes |
| K85.32 | Drug-induced acute pancreatitis with infected necrosis | ✓ Yes |
| Sequencing Rule: Sequencing K85.3x goes first as the principal/first-listed diagnosis. The T-code (adverse effect) sequences after. The T-code must include the seventh character ‘A’ (initial encounter), ‘D’ (subsequent), or ‘S’ (sequela) — don’t leave it off. |
K85.8x / K85.9 — Other Acute & The Code You Should Never Submit
K85.8x covers legitimate ‘other’ causes: trauma, hypertriglyceridemia, hypercalcemia, post-ERCP pancreatitis, hereditary, and autoimmune pancreatitis. These are real, billable codes with valid fifth-digit extensions.
| Code | Description | Billable |
| K85.80 | Other acute pancreatitis without necrosis or infection | ✓ Yes |
| K85.81 | Other acute pancreatitis with uninfected necrosis | ✓ Yes |
| K85.82 | Other acute pancreatitis with infected necrosis | ✓ Yes |
| Never Use K85.9: K85.9 is a billing dead end. It’s the unspecified parent code, explicitly marked as non-billable. If you submit it on a claim, you’re either going to get a rejection or a payment that gets clawed back on audit. Always push for a five-character specific code. |
K86 — Chronic Pancreatitis and Complications
Chronic pancreatitis codes don’t carry the fifth-digit necrosis extension that K85 codes do — the chronicity itself implies ongoing damage. But the etiology still matters for code selection, and the associated complications need their own codes.
K86.0 — Alcohol-Induced Chronic Pancreatitis
Long-term alcohol use is the leading cause of chronic pancreatitis in the United States. When the physician explicitly documents alcohol as the causative factor — not just as a comorbidity — this is the right code. The same documentation rule applies here as with K85.2x: a causal statement must be present, not just a history.
| Coder Tip: Add F10.xx for alcohol use disorder when documented. And if exocrine insufficiency is also present — which it commonly is in advanced chronic pancreatitis — add K86.81 as a secondary code per the ‘code also’ instruction. |
K86.1 — Other Chronic Pancreatitis
This is one of the most frequently assigned chronic pancreatitis codes — it covers autoimmune pancreatitis, hereditary pancreatitis, obstructive chronic pancreatitis from ductal stricture, and idiopathic chronic pancreatitis. It’s also the code that goes on the chart when alcohol is NOT the documented cause, or when causality isn’t clearly stated.
It’s also the code you add as a secondary diagnosis in acute-on-chronic presentations — more on that in the next section.
K86.2 — Pseudocyst of the Pancreas
When a pancreatitis episode leaves behind a fluid-filled collection with a fibrous wall, it must be captured separately in addition to the underlying pancreatitis code. Pseudocysts can persist weeks after the acute episode resolves and may require drainage procedures, so don’t let them fall off the claim.
K86.81 — Exocrine Pancreatic Insufficiency (EPI)
As chronic pancreatitis destroys the enzyme-producing cells of the pancreas, the patient can no longer digest fat and protein adequately. This is a billable, specific diagnosis that pairs with K86.0 or K86.1 as a secondary code when documented. It matters clinically for treatment (enzyme replacement therapy) and for coding completeness.
Acute-on-Chronic Pancreatitis: The Dual-Code Scenario
This is one of the most commonly undercoded scenarios in gastroenterology. A patient with established chronic pancreatitis comes in with an acute flare — severe pain, elevated lipase, the whole picture. You need two codes.
| Principal Diagnosis K85.xx The acute episode — etiology and severity determine the specific subcategory and fifth digit | Secondary Diagnosis K86.1 The chronic underlying condition — documents the full clinical picture and case complexity |
The acute code sequences first because that’s what drove the admission. The chronic code follows to capture the full clinical picture. Missing the chronic component isn’t just an accuracy problem — it can understate the complexity of the case and affect quality reporting metrics.
| Warning: Documentation requirement: Both the acute episode and the underlying chronic disease must be documented by the attending physician in the current encounter note — not just referenced in the history. If the chronic pancreatitis is only in the past medical history and not acknowledged in the current note, query before adding it. |
DRG Mapping: Where Your Coding Decisions Hit the Bottom Line
All pancreatitis codes — whether K85 or K86 — map to the same MS-DRG cluster. But which tier you land in depends entirely on what you code alongside the pancreatitis diagnosis.
| DRG | Description | Reimbursement | What Gets You Here |
| 438 | Disorders of Pancreas Except Malignancy with MCC | Highest | Infected necrosis (.x2), sepsis, acute respiratory failure, multi-organ dysfunction |
| 439 | Disorders of Pancreas Except Malignancy with CC | Mid-tier | Acute kidney injury, pleural effusion, uninfected necrosis (.x1), new-onset diabetes |
| 440 | Disorders of Pancreas Except Malignancy without CC/MCC | Base rate | Uncomplicated pancreatitis with no significant comorbidities coded |
A patient admitted with acute pancreatitis who develops acute kidney injury during the stay gets coded with N17.9 as a secondary diagnosis. That’s not upcoding — that’s complete, accurate coding. Failing to capture it drops a legitimate CC, potentially reducing reimbursement by thousands of dollars per case.
| CDI collaboration tip: Pancreatitis is a high-value CDI opportunity. Proactively review all pancreatitis admissions for documented complications (AKI, sepsis, respiratory involvement, necrosis status) and query attending physicians when these conditions are present but not explicitly linked to the pancreatitis diagnosis. |
The 5 Billing Mistakes That Show Up on Pancreatitis Claims
In practice, pancreatitis claims have a predictable set of errors that show up on audits and in denials. Here are the five most common — and what to do instead.
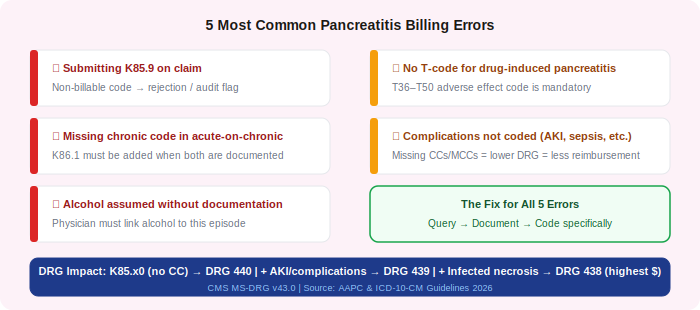
Error 1 — Submitting K85.9 on the claim
The unspecified parent code is the single most frequent error on pancreatitis claims. K85.9 is explicitly non-billable and will cause rejections or audit flags.
| ✓ Fix: Query the physician for etiology and necrosis/infection status. Use the most specific five-character code available. |
Error 2 — Missing the chronic component in acute-on-chronic cases
Patients with known chronic pancreatitis who present acutely are a dual-code scenario every time. Coding only the acute episode leaves an incomplete picture and understates case complexity.
| ✓ Fix: When chronic pancreatitis is documented in the current encounter note, add K86.0 or K86.1 as a secondary diagnosis alongside the acute K85.xx code. |
Error 3 — Assuming alcohol caused it without a causative statement
A patient with a 15-year history of heavy drinking presents with pancreatitis. It feels obvious. But ‘obvious’ isn’t documentation. Without a physician statement linking alcohol to this episode, you don’t have K85.2x.
| ✓ Fix Query the physician: ‘Does the patient’s current episode of acute pancreatitis appear to be related to their alcohol use?’ A one-line addendum is all you need. |
Error 4 — Forgetting the T-code on drug-induced pancreatitis
ICD-10-CM’s ‘use additional code’ instruction for K85.3x isn’t a suggestion — it’s a coding convention. Submitting K85.30 without the corresponding adverse effect T-code is technically incomplete and can trigger payer edits.
| ✓ Fix: Identify the specific drug, locate the appropriate T36–T50 adverse effect code, and sequence it after K85.3x. Include the correct seventh character (A/D/S) for the encounter type. |
Error 5 — Leaving concurrent complications off the claim
Severe pancreatitis rarely travels alone. Acute kidney injury, sepsis, pleural effusion, hyperglycemia, respiratory failure — these are real diagnoses that deserve their own codes. Missing them depresses the DRG weight.
| ✓ Fix : Review the entire inpatient record for conditions that meet the UHDDS definition of ‘additional diagnosis.’ When in doubt, query the attending to confirm the relationship to the pancreatitis. |
Accurate pancreatitis coding is not just about picking the right code — it is about protecting your revenue, staying audit-ready, and making sure every claim reflects the true clinical picture. If your practice needs expert support with ICD-10 coding or medical billing, the team at RevenueES specializes in exactly this — helping practices code with confidence and get reimbursed correctly, every time.
Documentation Checklist: What to Look for Before You Code
Before assigning any pancreatitis code, work through this checklist against the clinical record:
- Etiology stated? Does the physician explicitly name the cause (gallstones, alcohol, drug, trauma, idiopathic)?
- Acute vs. chronic specified? The clinical picture often makes this obvious, but the note must support the code choice.
- Necrosis documented? If severe, has the attending interpreted the CT findings and stated whether necrosis is present?
- Infection status addressed? For necrosis cases, is it infected or sterile?
- Chronic history acknowledged? If the patient has prior chronic pancreatitis, is it acknowledged in the current encounter note?
- Concurrent complications coded? AKI, sepsis, pleural effusion, diabetes — are all documented conditions being captured?
- Add-on codes required? Drug cause → T-code. Alcohol use disorder → F10.xx. EPI → K86.81.
Frequently Asked Questions
Is K85.9 ever acceptable on a claim?
No. The ICD-10-CM tabular list explicitly marks K85.9 as a non-billable, non-specific code. There is no clinical scenario where it’s the right choice for a submitted claim. If you find yourself considering it, that’s a signal to go back to the documentation and query the physician for specificity.
Can I code both acute and chronic pancreatitis on the same claim?
Yes, and you should in acute-on-chronic presentations. Assign the acute code (K85.xx) as the principal diagnosis reflecting the reason for the encounter, and add K86.0 or K86.1 as a secondary code. Both must be documented in the current encounter note by the attending physician.
My patient has pancreatitis caused by high triglycerides — what code do I use?
Assign K85.80 (other acute pancreatitis — appropriate fifth-digit variant based on severity) and add E78.1 (pure hyperglyceridemia) as a secondary code per the ‘use additional code’ convention. Hypertriglyceridemia-induced pancreatitis falls under the ‘other’ category since there’s no dedicated subcategory for it in K85.
What about post-ERCP pancreatitis?
Post-ERCP pancreatitis is coded as a complication of the procedure. In many cases K85.80 is used with an additional code indicating the complication was procedure-related — verify with your organization’s coding compliance guidelines and current payer policies.
Does the order of K85.xx and K86.1 matter on an inpatient claim?
Yes. For inpatient claims, the principal diagnosis is the condition established after study to be chiefly responsible for the admission. In most acute-on-chronic presentations, the acute episode (K85.xx) is what drove the admission and should sequence first.
Key Takeaways
| 1. Every billable pancreatitis code needs five characters. If yours has fewer, stop and find the right one. |
| 2. K85.9 is not a fallback option. It’s a non-billable placeholder. Never submit it on a claim. |
| 3. The fifth digit (.x0 / .x1 / .x2) is where DRG value lives. Infected necrosis is a Major Complication. |
| 4. Causation must be stated, not implied. Alcohol history doesn’t equal K85.2x. A physician statement does. |
| 5. Dual-code every acute-on-chronic case. K85.xx first, K86.1 second — both in the current encounter note. |
| 6. Drug-induced pancreatitis always needs a T-code companion. The ‘use additional code’ instruction isn’t optional. |
| 7. Concurrent complications change your DRG. Capture every documented secondary diagnosis. |
| 8. When in doubt, query. A clear physician addendum is always better than a defensible guess. |
| Sources & Disclaimer: This article was written using the 2026 ICD-10-CM Official Guidelines for Coding and Reporting (effective October 1, 2025), AAPC Codify, CMS MS-DRG v43.0, and the ICD-10-CM Tabular List. All codes and DRG assignments are current as of the publication date. Always verify against your organization’s internal compliance guidelines and current payer contracts before submitting claims. |



